Herpes is a herpes virus infection that is not dangerous to humans, but can cause a lot of trouble for cats themselves. Murkoshi specialists warn that poor-quality treatment or lack thereof can lead to serious complications and even (very rarely, but still) death. We will tell you further how to recognize herpes at an early stage and provide qualified assistance.
1) Herpes – what is it?
2) Routes of infection
3) Signs of herpes
4) Diagnostics
5) Treatment
6) Disease prevention
Herpes - what is it?
Translated from Greek, this word means a creeping, spreading skin disease, which is characterized by the presence of blisters on the skin and mucous surfaces. Without treatment, it leads to a more serious disease – rhinotracheitis.
The most common type of virus is herpesvirus-1 (FHV-1), which is very common and highly contagious. It can either be acute or become chronic.
The acute form lasts about 14 days. Usually the pet recovers during this time. If left untreated, pneumonia can become a complication.
Read more about pneumonia: Symptoms and treatment of pneumonia in cats
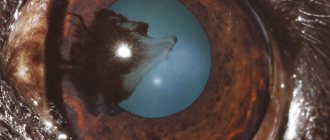
The chronic form lasts about 6 weeks. Complications may include panophthalmia, ulcerative keratitis and blindness.
Animals with weakened immune systems are most often at risk. Herpes in a kitten can appear at an early stage of its life, and it can become infected from its mother. The unprotected body of babies (immunity has not yet developed), up to 1 month old, cannot resist such a disease. In this case, kittens, unfortunately, usually die.
There is a high probability of herpes in cats that have experienced stress.
Mechanism of disease development
Once on the mucous membranes of the respiratory tract, the virus penetrates the epithelial cells and reproduces, causing their death and desquamation. Subsequently, an inflammatory reaction occurs, first small and then more extensive areas of necrosis are formed on the surface of the mucous membrane. Adsorbed on leukocytes, the virus enters the blood and causes viremia, manifested by general depression of the animal and fever.
When the virus penetrates the placental and blood-brain barriers, damage occurs to the brain, placenta, uterus and fetus. The pathological process of infectious rhinotracheitis largely depends on complications of opportunistic microflora, manifested by the development of bronchitis, pneumonia, gastritis and enteritis. The course of the disease is aggravated by mixed infection with adenoviruses and panleukopenia.
Routes of infection
Infection of herpes in cats occurs through contact and sexual contact. A domestic cat can also catch the virus - from the owner’s clothes and shoes. The main sources of spread of the herpes virus are discharge from the cat’s nose and mouth. A person who pets a sick animal can “reward” their pet with this virus. Feline herpes can exist for a long time in the environment, the main thing is that there is sufficient humidity. It is located in the ground and grass, so any animal can become infected.
Treatment eliminates all symptoms of the disease, but the virus itself remains in the body. It is completely safe for others, but under favorable conditions (stress, factors that reduce immunity, etc.), herpes is activated again. Herpes in cats accumulates most of all in the trigeminal nerve. The Murkoshi team warns that the cat will release the virus into the air for about 6 months after recovery.
Pathogen
A large family of herpes viruses affects not only mammals, but also birds, as well as reptiles, fish and amphibians. The peculiarity of infectious diseases caused by viruses from this family is an acute course, passing into a dormant stage and the absence of characteristic signs of being in the body until a certain point.
The feline rhinotracheitis virus Feline viral rinotracheitis-2 reproduces well in the mucous membranes of the pharynx and nasal passages, as well as in the tonsils and trachea. The development of rhinotracheitis is also diagnosed in the conjunctival membranes, which is associated with an excellent environment for the nutrition and reproduction of foreign microorganisms.
Herpesvirus infection has the ability to maintain its virulence in acidic environments, but is sensitive to high temperatures.
Deactivation of microorganisms occurs when they are exposed to ether, chloroform, formaldehyde, phenols and sodium hydroxide. These chemicals are widely used to disinfect premises and care items for a pet that has become infected, as well as to prevent infection.
It has been proven that some factors indirectly influence the development of herpesvirus in cats. These include:
- hypothermia of the animal;
- improper conditions of detention;
- violations in the diet (lack of necessary nutritional components).
The main route of transmission of the feline rhinotracheitis virus is airborne. That is, infection occurs when a sick animal comes into contact with a healthy one. There is also a nutritional route, which involves infection through feed. But this assumption has not been proven.
After suffering rhinotracheitis, the cat can spread the infection for quite a long time. Unfavorable conditions after infection and complete recovery of the cat can provoke a relapse of the disease. In clinical practice, cases are described when a recovered animal is completely freed from infection. But such cases are rather the exception to the rule.
Diagnostics
You cannot diagnose herpes in a kitten on your own. Many other diseases have the same symptoms. Only a doctor can make the correct diagnosis. Do not forget to tell the specialist when and how the disease began to develop.
Read about proper communication with a veterinarian: 5 rules for effective interaction with a veterinarian
The veterinarian will examine the animal for ulcers. He will take an antibody test, blood tests, scraping of secretions for the presence of the virus and begin treatment.
Diagnosis
Based on the analysis of epidemiological, clinical data and laboratory test results (PCR) of discharge from the mouth, nose, eyes and virus isolation in cell culture. To clarify the diagnosis, a neutralization reaction (RN) is performed in a culture of kitten kidney or lung cells, and the selective persistence of the virus at different temperatures is also taken into account.
For RN, a standard virus and inactivated serum are used, and it is taken into account on the 3rd day. In cats with runny nose, conjunctivitis and rhinitis, in addition to the rhinotracheitis virus, picornaviruses, reoviruses, mycoplasmas and chlamydia can be isolated. Often feline rhinotracheitis occurs simultaneously with calicivirus infection and panleukopenia.
Treatment
To date, there are no methods that can completely cure herpes in a cat. The main task of a specialist is to eliminate symptoms and prevent relapses. The following types of drugs are used for treatment:
1) General antiviral drugs.
2) Drops for the nose and eyes.
3) Strengthening drugs.
4) Antibiotics that fight secondary infections.
5) Painkillers.
To protect the mucous membrane from further development of the disease, Acyclovir ointment is used. The procedure is carried out up to 6 times a day for a week. Before applying the ointment, treat the affected areas with a cotton pad soaked in Miramistin.
Acyclovir tablets are prescribed for general antiviral therapy. This drug should be given with caution to cats with impaired liver function. The exact dosage will be prescribed by your veterinarian. After taking the drug, it is necessary to monitor the pet’s condition for some time.
The immunity of a kitten with herpes is greatly weakened, therefore, good vitamin therapy is needed. And to prevent the development of inflammation, antibacterial drugs are used, for example, Tylosin.
Prevention
It is based on strict adherence to veterinary and sanitary rules, timely diagnosis, isolation of sick and suspected cats, symptomatic treatment aimed at eliminating inflammation in the respiratory system and dehydration of the body. For active immunoprophylaxis of cats, an attenuated vaccine from the F-2 strain is used.
Animals aged from 3 months to 3 years are vaccinated. After 3 weeks, vaccination can be repeated. Immunity lasts up to a year. Animals are provided with optimal living conditions and are provided with nutritious food. To disinfect premises and care items, use 2% solutions of formaldehyde and caustic soda, as well as bleach and Virkon S preparations.
Recommendations for caring for a sick animal
Once the veterinarian has confirmed the diagnosis, the cat should be placed in a warm room, making sure that there are no drafts in the room. She needs special nutrition during treatment. If your pet has no appetite, you can stimulate it using any strong-smelling products.
A sick cat must be isolated from other pets. To make it easier for her to breathe and also to clear her stuffy nose, it is recommended to do inhalations or periodically keep the animal in a steamed bathroom for a while (to do this, turn on the hot water and close the door tightly).
The tray and bowls for food and water should always be clean. The cat needs to periodically rinse its nose, as accumulated mucus makes breathing difficult.
To destroy the virus in the premises, all surfaces are wiped with a disinfectant solution. To do this, mix bleach and water in a ratio of 1:32 (to one part bleach, 32 parts water). Objects and surfaces that should not be exposed to chlorine solution can be treated with soapy water. There are special disinfectants for treating upholstered furniture.
Diet
If the cat has been fed only dry food all the time, for the period of treatment it is better to switch it to wet food from the same manufacturer or select a special line of food rich in vitamins and minerals. This will help restore immunity faster. If a furry patient has a natural diet, his menu should be supplemented with the following dishes:
- liquid soup;
- porridge;
- meat puree (chicken and beef);
- pate processed with boiling water;
- boiled fish;
- vegetable puree.
Such nutrition will replenish the body with essential vitamins.
It is necessary to change the water two to three times a day; it must be bottled or filtered. Tap water should not be given. Until the animal recovers, you should not give it cat treats from pet stores. Eliminate food from the host’s table completely, this will only harm your health.
The key to a cat’s health is a timely visit to the veterinarian
Current issues of severe herpetic infection in adults
Currently, the number of patients with recurrent herpes infection caused by herpes simplex viruses (HSV) types 1 and 2 of various localizations is steadily increasing. The most common localization in adults is anogenital and labial. Many issues of the pathogenesis and treatment of severe and extremely severe herpesvirus infection are still not resolved.
The HSV species belongs to the family Herpesviridae, subfamily L-Herpesviridae, a species of HSV. There are two main types of virus - HSV 1 and HSV 2. Infection is possible with either one or two types of pathogen. HSV is capable of invading various cells of the human body: skin cells, mucous membranes of the urogenital and gastrointestinal tracts (GIT), respiratory tract, central and peripheral nervous system, liver, vascular endothelium, as well as blood cells - lymphocytes, etc. [ 1]. The place of permanent residence (lifelong persistence) of HSV is the paravertebral sensory ganglia. HSV is transmitted by direct contact; the pathogen can be transmitted through household contact and vertical routes (from mother to fetus), as well as through transfusion and parenteral routes through instruments during surgical interventions, dental procedures, etc.
As you know, most people are infected with HSV. The primary immune response to infection occurs latently or with herpetic eruptions with a local and general inflammatory reaction. In individuals with a normal immune response, HSV multiplication (replication) is under immunological control, and relapses are extremely rare or do not occur throughout life. The antiviral defense of the body involves nonspecific defense factors that destroy or block viruses: macrophages and other cells producing interferons (IFN) α, β and γ, a number of interleukins (IL) (tumor necrosis factor (TNF), IL-6, etc.) , natural killer cells and factors that form a specific immune response against a particular virus: cytotoxic T lymphocytes (CTL) (CD8+ T lymphocytes) and B lymphocytes, responsible for the production of specific antibodies that block the replication of the virus and viruses located outside the cell. For adequate functioning of these cells and maintaining the immune response, appropriate production of IFN and IL is necessary.
Under the influence of various exogenous and endogenous factors that damage the immune system, control over viral replication may weaken and, accordingly, the development of relapse. Recurrence of HSV infection can be triggered by other infectious diseases, hypothermia, excessive insolation, mental or physical stress, intoxication of various origins, including alcohol consumption, cyclical changes in hormonal status (menstruation), especially with an imbalance of hormone levels in women, sudden changes in climatic zones and etc.
With long-term chronic infection, viruses have a multifaceted adverse effect on the human immune system. HSV directly damages cells of the immune system (lymphocytes, macrophages and natural killer cells). By synthesizing suppressor proteins and chimeric proteins, viruses inhibit many immune reactions: HSV can block the action of IFN, disrupt the recognition of infected cells and other protective reactions. In addition, the high mutational activity of the viral genome also contributes to the escape of the virus from immunological control.
Chronic, often recurrent HSV infection can provoke the development of autoimmune conditions (antiphospholipid syndrome, autoimmune thyroiditis, autoimmune vasculitis, etc.). In addition, when HSV is integrated into the genetic apparatus of cells, neoplastic transformation of cells is possible. Thus, HSV is one of the increased risk factors for developing body and cervical cancer and other cancers. Also, HSV infection is one of the leading causes of spontaneous abortions, premature births, and the birth of children with pathologies of the central nervous system and internal organs. HPHI is associated with many “diseases of civilization” - atherosclerosis, coronary heart disease in people under 50 years of age, etc. Severe HPHI can be a marker of cancer and AIDS [7].
Depending on the number and severity of relapses, mild, moderate and severe courses of the disease are distinguished (Table 1).
In severe cases of HSV infection, the simultaneous appearance of several lesions (for example, in the genital area, lips, wings of the nose), as well as the sequential occurrence of rashes of different localization (one relapse against the background of another), the duration of the exacerbation can reach 16–20 days. At the site of the rash, patients feel heat, burning, pain, tension and/or itching of the skin. A group of bubbles filled with transparent content appears on the infiltrated skin. Bubbles can merge into a continuous multi-chamber element. Their transparent contents then become cloudy. The bubbles subsequently open, forming small erosions, or dry out and turn into crusts. A secondary bacterial infection may develop. With relapses, HSV often affects the same areas of the skin. As a rule, with severe infection, the physical and mental condition of patients worsens significantly. In some patients, during the period of relapse, weakness, fever, chills, myalgia, cephalalgia, arthralgia, irritability, sleep disturbance, emotional lability increase or appear; severe depressive states requiring drug correction may also develop. According to US health authorities, HSV infection of anogenital localization is the cause of depression and suicide in approximately 10% of cases. The severe course of the genital form of HSV infection with frequent relapses leads to disruption of the patient’s normal sexual function; the disease often creates conflict situations in the family and at work. Treatment of patients with severe HSV infection is a complex task and should include both drug therapy and psychological adaptation of the patient.
In patients with severe HSV infection, in most cases there is no persistent and significant clinical effect in response to episodic courses of combination therapy (antiviral and immunotropic drugs, restorative drugs). As a rule, such patients change many medical institutions in search of adequate help.
As the disease progresses, many adverse reactions to medications or intolerance to them appear; in some cases, HSV resistance to acyclovir, IFN-a, and other drugs develops. Immunostimulants used empirically may provide relief when taken, but in many cases they are ineffective and even worsen the clinical course of the disease. Manifestations of secondary immunodeficiency worsen, other infections occur, subdepressive states turn into persistent mental disorders, patients lose faith in recovery and in the ability of modern medicine to help them.
To develop modern approaches to the treatment and control of HSV infection and a more in-depth understanding of the pathogenesis of the disease, we studied the state of various parts of the antiviral defense and the cytokine system in patients with severe and extremely severe HSV infection of anogenital and labial localization, as well as the degree of infection ( systemicity of the disease) and the frequency of combination with other herpesvirus infections.
We examined 102 patients suffering from severe HSV infection for more than 2 years (28 men and 74 women, average age 34 ± 1.5 years) and having a relapse rate of more than six per year.
Moreover, 60 patients had from 6 to 11 relapses of HSV infection per year, and 42 patients had from 12 to 20 relapses. In most patients, anogenic or mixed localization of herpes predominated. The average duration of severe disease was 9.3 ± 1.2 years. The control group consisted of 32 practically healthy volunteers (14 men and 18 women, average age - 32 ± 1.6 years). The analysis of a number of parameters studied included the results of an examination of patients with a mild course of the disease (36 people - 10 men, 26 women, average age - 33.4 ± 2.1 years, with a relapse rate of 2.9 ± 0.8 per year). During relapses, the patients' complaints were characteristic. Depression, irritability, memory loss and other disorders of the physical and mental state and cognitive functions were common.
Many patients had a history of repeated courses of antiviral and/or immunotropic therapy, which had an ambiguous effect: either a short-term positive effect on the course of HSV infection, or worsening and development of relapse during or after the cessation of immunocorrection. Such anamnestic data reflect the severity of immune deficiency and the inadequacy of empirical therapy without assessing the immune status and individual selection of immunocorrectors, as well as restorative therapy - immunorehabilitation [5].
When examining patients with severe HSV infection, many markers of secondary immunodeficiency were identified in the form of chronic infectious and inflammatory diseases of various localizations, with a mixed nature of the microflora and, in most cases, its resistance to repeated courses of antibiotic therapy. Of 102 patients with chronic severe HSV infection, the following were identified:
- 86.3% had chronic recurrent diseases of the respiratory tract (chronic pharyngitis, chronic tracheitis, chronic laryngitis, chronic bronchitis, chronic sinusitis, repeated otitis);
- 88.2% had chronic recurrent diseases of the urogenital tract of mixed origin (cystitis, urethritis, vulvovaginitis, adnexitis, salpingoophoritis, prostatitis);
- 50–70% have astheno-vegetative and astheno-depressive syndrome, the formation of chronic fatigue syndrome;
- 91.2% had dysbiosis of the intestinal flora, chronic inflammatory diseases of the gastrointestinal tract (chronic enterocolitis, chronic gastroduodenitis);
- 25–30% have pseudo-allergic skin reactions (itching, urticaria, dermatitis).
These data indicate the need for an integrated approach to the treatment of severe HSV infection, taking into account the complications of secondary immunodeficiency.
The presence of HSV infection was confirmed based on medical history, clinical data, and the detection of HSV deoxyribonucleic acid (DNA) by polymerase chain reaction (PCR) in discharge from the rash. The study of immune status included determination of the main subpopulations of lymphocytes CD3+, CD4+, CD8+, CD72+, CD16+, activation markers of lymphocytes of the major histocompatibility complex - HLa-DR+, CD11b in peripheral blood using monoclonal antibodies. The content of immunoglobulins (Ig) a, M, G, and circulating immune complexes (CIC) in blood serum was also determined. The functional activity of neutrophils—the production of reactive oxygen species that provide bactericidal activity—was determined using the nitroblue tetrazolium test (NBT test). The stimulated NBT test was studied by incubation in vitro with a Staphylococcus aureus culture. Interferon status was assessed by the level of serum IFN and production of IFN a by leukocytes upon stimulation with New Castle disease virus and IFN ( upon stimulation with phytohemagglutinin. Quantitative content of cytokines (IFN α, IFN γ, TNF α, IL-1β, IL-2, IL-4 IL-6) in blood plasma/serum was determined by enzyme-linked immunosorbent assay (ELISA) using test systems (ProCon, St. Petersburg, and Vector-Best, Novosibirsk).
In addition, a PCR study of biological materials was carried out for the presence of DNA of HSV types 1 and 2 and other herpes group viruses: cytomegalovirus, human herpes virus (HHV) type 6, Epstein-Barr virus. The amplification programs we used made it possible to detect viral DNA at a level corresponding to their active replication. The presence of active viral replication was confirmed by semi-quantitative PCR studies and serological tests.
As a result of the study, laboratory signs of secondary immunodeficiency were found in patients with severe HSV infection.
| Figure 1. Frequency of detection of different IgG values in patients with severe HSV infection |
Thus, the majority of patients (91%) did not have an adequate increase in IgG production in response to recurrent HSV infection (Fig. 1). With a recurrence rate of HSV infection of 6–11 relapses per year, a low level of IgG was detected in 25% of patients; with a frequency of 12–20 relapses per month, it was detected in 64.3% of patients. More than 70% of patients had an increased level of CEC by 1.5–2.0 times the normal level. It is known that long-term circulation of CEC can lead to their deposition on the vascular endothelium and serve as one of the factors in the formation of autoimmune pathology.
In the majority of patients with severe HSV infection (70%), disturbances were found in the system of natural and/or specific cytotoxicity (Fig. 2) - a decrease in the content of mature activated natural killer cells CD16+ (less than 11%), T-killers and/or CTLs CD8+ (less than 27%). It is important to note that a pronounced decrease in the level of CD8+ (which also includes suppressor cells) in most cases was combined with an increase in the level of CD4+ and the immunoregulatory index, which is a risk factor for the formation of autoimmune processes. As is known, natural and specific cytotoxicity systems play a leading role in antiviral defense.
| Figure 2. Frequency of detection of disturbances in the system of natural and specific cytotoxicity in patients with severe HSV infection (n = 102) |
In patients with severe HSV infection during relapse, the number of natural killer cells was significantly lower than normal and 2 times lower than the average for persons with mild disease. In almost half of the patients with HSV infection, the identified disorders were combined with disimmunoglobulinemia and deficiency of IgG production. The level of HLa-DR+ lymphocytes, which reflect the production of IL-2 and carry the DR+ receptor, necessary for recognizing virus-infected cells and other immune reactions, was reduced in 39% of patients with HSV infection (its increase was noted only in 17.4% of patients).
The detected disturbances in cytotoxicity systems and their activation markers during HSV infection indirectly indicate an insufficient level of production of IL-2 by T-helper type 1 cells, one of the most important links in the cytokine network, necessary for a complete antiviral immune response.
When studying the functional state of neutrophils in patients with severe HSV infection, an increase in the spontaneous NBT test was detected in almost half of the cases. However, the parameters of the stimulated NBT test and the stimulation index, on the contrary, were significantly reduced in the majority of patients, which indicates that their reserve abilities of neutrophils were depleted.
When studying the interferon status of patients during an exacerbation of HSV infection, differences were identified between mild and severe disease. Thus, the level of serum IFN in patients with mild disease was increased by 2 times compared to the control group (p < 0.05). In severe cases of infection, on the contrary, relapse was accompanied by a low level of serum IFN. The stimulated production of IFN a and IFN g was also reduced, and to a significantly greater extent precisely in cases of severe HSV infection.
Thus, the majority of patients with HSV infection showed severe deficiency of the interferonogenesis system, which correlates with data on the depletion of the reserve abilities of neutrophils in these patients.
We also studied the content of the main pro-inflammatory ILs (IL-1β, TNF α, IL-2 and a number of other ILs) in the blood serum during the period of relapse and during the period of illness outside of rashes. It turned out that in patients with severe HSV infection on days 2–3 of relapse there is no adequate response from pro-inflammatory ILs. In the majority of patients (90%), insufficiency of IL production was detected, and in approximately 10% of patients the studied ILs were not detected in the blood. It should be noted that during the non-rash period, a long-term increase in the level of one or two types of cytokines was also detected.
During a PCR examination of patients with severe HSV infection (the main group), the Epstein–Barr virus (in 76.5% of cases) and HHV type 6 (in 63.5% of cases) were most often found in the oropharyngeal area. Cytomegalovirus infection was detected in 11.0% of patients in this group (in the epithelial cells of saliva, urethra, cervical canal, and in urine sediment). In cases of mild HSV infection (comparison group), the DNA of the above viruses was detected significantly less frequently (Table 2). In general, in severe cases of the disease, the proportion of patients with HSV monoinfection was only 5%, and in mild cases it was about 72% (Table 3).
Thus, it was found that in 95.6% of patients with HSV infection with severe disease, other viruses of the herpes group actively replicate, which allows us to consider this form of the disease as a mixed viral severe infection.
Above, we noted the serious problems that arise in the treatment of HSV infection. As our studies have shown, a major role in the pathogenesis of the disease is played by secondary immunodeficiency, often combined with impaired cytokine production, as well as the presence of a mixed viral herpetic infection. In addition, against the background of these powerful interrelated factors, infectious and inflammatory diseases of the mucous membranes are added to the underlying disease. As a rule, these factors are not taken into account when treating patients with HSV infection.
Treatment of HSV infection should include suppression of viral replication during the period of exacerbation, as well as the formation of a complete immune defense in order to prevent relapses. Previously, we outlined in detail the principles of treatment for IPHI [3, 4]. To stop the exacerbation of herpes infection, acyclic nucleotides (acyclovir, valacyclovir, famciclovir) are used, the action of which is associated with the ability to disrupt the process of HSV replication at the stage of viral DNA synthesis and assembly of viral particles. The effectiveness of acyclic nucleotides depends on their bioavailability, the sensitivity of the virus to the drug, the adequacy of the dose, the duration and frequency of treatment, and the timing of the start of treatment. Prescribing these drugs from the first day of relapse (acyclovir - in a daily dose of at least 1000–1600 mg) helps to quickly stop it (Table 4).
For patients with HSV infection with frequent relapses (six or more relapses per year), in order to prevent them, suppressive administration of acyclic nucleotides is recommended for a long time, which can lead to drug remission during the treatment period. At the same time, a decrease in the frequency of relapses after cessation of treatment (compared to the period before therapy) is observed in only 20% of patients [2]. Acyclic nucleotides of the new generation - valacyclovir and famciclovir, compared to acyclovir, have higher bioavailability with the possibility of two- and three-fold administration, but these drugs are very expensive.
After a year of continuous antiviral therapy, treatment is interrupted to assess the number of relapses. For patients whose relapse rate continues to be unacceptably high, it is advisable to restart treatment [2]. With long-term or frequent therapy with acyclic nucleotides, side effects (gastrointestinal pain, dizziness, etc.) may occur; in some cases, virus resistance to this group of drugs develops. Agents that suppress HSV replication also include glycyrrhizic acid (found in licorice), IFN α (reaferon, viferon, realdiron, etc.) and inducers of its synthesis (amixin, cycloferon, ridostin, poludan, etc.). In case of severe and prolonged course of HSV infection, in the case of a course of use of these drugs during monotherapy, an insufficient clinical effect is noted; with long-term use, known side and undesirable effects develop. IFN a represents only part of the antiviral defense of the immune system and cannot replace its other parts if they fail. In addition, as mentioned above, herpes viruses are able to block the action of IFN α. As clinical experience and our data show [5, 6], the use of immunocorrectors without assessing the immune status, individual selection and control of their action is ineffective or can lead to increased immune dysfunction or hyporeactivity of a number of immune components due to inadequate stimulation. It should be emphasized that the prescription of drugs for topical use (ointments containing acyclovir, sodium foscarnet; epigen intim spray (glycyrrhizic acid), bonafton) is only auxiliary in nature, since blistering rashes on the skin are only one of the manifestations of severe HSV infection. The herpes virus, as shown in the literature and our experience, can replicate in other cells and organs (in the oropharyngeal region, lymph nodes, rectal mucosa, etc.). In addition, our research shows that severe HSV infection is, in fact, not a mono- but a mixed viral infection that develops against the background of secondary immunodeficiency, which changes the view on the examination and treatment of these patients.
We will indicate the principles of examination and treatment of patients with severe HSV infection.
Necessary examinations:
- General clinical examination - for the presence of concomitant diseases and infections (respiratory organs, gastrointestinal tract, urogenital tract - ultrasound examination, magnetic resonance therapy, etc.).
- PCR to detect HHV 4 and 6, cytomegalovirus, hepatitis viruses and intracellular infections (chlamydia, etc.).
- Complete immunological examination.
- Study of hormonal status.
- Study of tumor marker levels over time.
- Carrying out rheumatic tests in dynamics.
- If necessary, oncology search.
Treatment of exacerbation:
- Acyclic methods (acyclovir, valacyclovir, famciclovir) orally for 7–14 days.
- Locally: bonafton, acyclovir, Zovirax, Epigen, etc.
- Detoxification - according to the severity of the condition (enterosorption, plasmapheresis, hemosorption).
- Replacement complex immunotherapy (intravenous Ig, thymic peptides, IFN α and γ, IL preparations).
- Antioxidants comprehensively according to survey data.
- Metabolics.
- Vitamin therapy.
- Laser therapy.
- If necessary, treatment in a hospital.
Treatment of concomitant diseases: treatment and correction of identified concomitant disorders, diseases - chronic infections of the respiratory tract, urogenital tract and gastrointestinal tract, dysbacteriosis, hormonal dysfunctions, metabolic syndrome, depression, etc.
Relapse prevention:
- Eliminate provoking factors (occupational hazards, cold, nervous and physical overload, alcohol abuse, etc.).
- Eliminate other factors that suppress the immune system (poor diet, lack of sleep, smoking, physical inactivity, etc.).
- According to the examination, repeated courses of replacement immunotherapy, other types of immunocorrection, immunorehabilitation.
- The use of IFN, IFN inducers, glycyrrhizic acid preparations, isoprenazine (bivalent drugs with antiviral and immunotropic effects) in a course regimen.
- Prolonged courses of abnormal nucleotides.
- Antioxidants.
- Vitamin therapy, metabolism.
- Dynamic observation.
In conclusion, it must be emphasized that the heterogeneity of disturbances in the immune system during HSV infection requires a differentiated approach to their correction. It seems important to further study the cytokine response in dynamics during severe disease. It is advisable to study the effect of cytokines IL-2 (roncoleukin), IFN γ (gammaferon, ingaron) and other drugs, accompanied by individual selection of treatment regimens, on the course of the disease.
Literature
- Khakhalin L.N. Herpes simplex viruses in humans // Consilium Medicum. 1999. T. 1. No. 1. P. 5–18.
- European standards for the diagnosis and treatment of sexually transmitted diseases. M.: Medical literature, 2003. pp. 102–110.
- Malashenkova I.K., Didkovsky N.A. Principles of immunocorrective therapy for secondary immunodeficiencies associated with chronic viral-bacterial infection // Russian Medical Journal. 2002. T. 10. No. 21. P. 973–977.
- Malashenkova I.K., Didkovsky N.A., Tanasova A.N., Shchepetkova I.N., Levko A.A. Principles of therapy for herpesvirus infection // Doctor.Ru. 2004. No. 4. pp. 26–30.
- Malashenkova I.K., Didkovsky N.A., Levko A.A. On the role of individual selection of immunocorrectors // Pharmateka. 2004. pp. 118–122.
- Levko A. A. The importance of individual selection of immunocorrectors in the complex therapy of chronic recurrent prostatitis caused by urogenital infection: abstract. dis. ...cand. honey. Sci. M., 2005.
- Shulzhenko A. E., Vikulov G. Kh., Tutushkina T. V. Herpetic infections - present and future // Difficult patient. 2003. No. 4. T. 1. P. 6–15.
N. A. Didkovsky , Doctor of Medical Sciences, Professor I. K. Malashenkova , Candidate of Medical Sciences Zh. Sh. Sarsaniya , Candidate of Biological Sciences A. N. Tanasova, I. N. Zuikova, I. A. Zuikov, N. M Khitrik Research Institute of Physico-Chemical Medicine, MMA named after. I. M. Sechenova, Moscow
Possible complications
If your cat is not treated, he may develop pneumonia, scars on his eyes, dry eye syndrome, and the animal may even go blind. The herpes virus often affects the lower lip and nose; ulcers and tissue necrosis may appear in these places. In some cases, the jawbone is destroyed. Rhinitis and conjunctivitis become chronic.
No more than 20% of cats die from herpesvirus. Kittens and adults with weak immune systems often develop pneumonia and die. If the disease develops in a pregnant cat, there is a high chance that a sick or dead kitten will be born.
In advanced cases, pneumonia may develop
How to help your pet recover faster
Also during treatment
It will be necessary
to change the
cat’s diet, which means that the pet will need to be given either liquid or semi-liquid food. Sometimes the animal is reluctant to accept such a change in its established diet, and in order to help it, you will have to literally force it at first.
To help the animal recover even faster, during the treatment process, antibacterial drugs can also be used in parallel along with immunomodulatory drugs, that is, those that will simultaneously increase the immune system of the animal’s entire body. In our veterinary center you can get all the necessary help, as well as consultation with an ophthalmologist.
Our veterinarian provides all the necessary services for treatment, examination and assistance to animals. You can always count on us, our help and the high qualifications of our team of veterinarians. Moreover, you, as an animal owner, should always remember that trying to cure a cat with little knowledge in this area is fraught with consequences.
Provide much-needed love, care and support through our team to your pet. We are always responsible for those we have tamed! We are always open to you and ready to advise on any questions you may have. Our veterinary center works for you and for your sake, because otherwise, why would we create it?! We will always provide due attention to your pet. For we understand how important it is for him to be healthy, to be happy himself and to continue to delight you with his shining and healthy eyes in the future.
Without a doubt, we understand that today people value their time very much, which is why our veterinary center provides such a service as a veterinarian visiting your home. This service is very convenient for residents of our metropolis, and your animal will receive even faster and more significant assistance. We do everything sterilely, having with us all the proper list of documents.